
Here is a general rule of thumb: every day of bed rest is worth three or more days of recovery. And you can modify those days if the patient is elderly, and more so when he/she is frail. Hospitalization for those in that group can result in new disabilities that often become permanent. The current study considers patients 65 or older who are hospitalized for PCR-proven seasonal flu – you know, the one no one thinks is bad, certainly not enough to get vaccinated against.
Functional assessment was made of the activities of daily living, otherwise known as ADL. [1] One hundred points meant entirely independent; 50 points meant the person required assistance, and; 0 points reflected total care. Functional decline was defined as a 9.25 point drop and was measured 30-days after discharge. Patients were also given a frailty score based upon several criteria.
The sample included 925 patients with acute viral respiratory illness and hospitalization 2011-2012. It was essential for every patient in the Canadian system. Mean age 79+, 56% women, 9.5% admitted from long term care. Of the total 37% or 346 had PCR-proven seasonal flu, the remaining patients were “the control.” The numbers get challenging to describe, but the chart makes understanding them easier. The changes reflect the findings 30 days after hospital discharge.
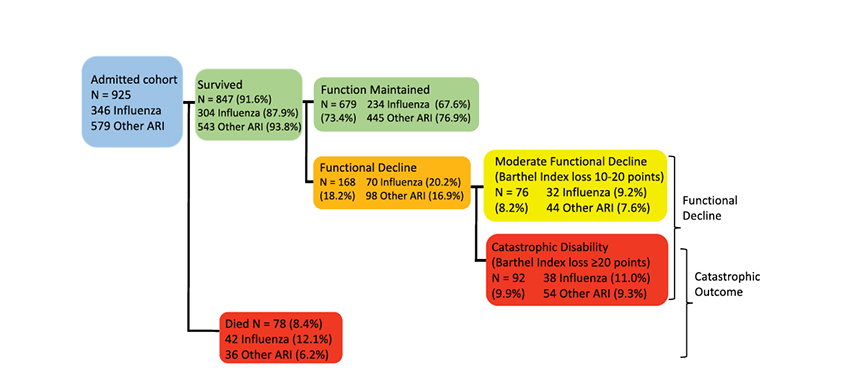
- Both groups “experienced a similar functional loss from baseline to admission” – more than 20 points for both groups
- Those with lower baseline function were more likely to die
- Among the survivors, nearly 20% were left with a moderate (10-20 point) or catastrophic (>20) decrease in their abilities.
- Baseline frailty resulted in more catastrophic disability. It was not so much that frails’ disease course was worse; their absolute drop in function was similar to the non-frail. The baseline for frail patients was already depressed, and a few points more was a much bigger problem for them. For the “most frail,” their disability increased by nearly 50%.
In this study of seasonal flu, 18.2% of patients experienced a significant functional loss. In many instances, it means that patients are not being discharged to home, but sent to rehabilitation or long-term care. They point out that length of hospitalization is usually taken as an outcome measure; shorter hospitalization durations mean quicker recovery. But here, the researchers flip the script, pointing out that longer lengths of hospitalization were risks in the outcome of more significant disability.
Being hospitalized for seasonal flu is not a benign process. It has, as evidenced by this study, real functional consequences. More importantly, these problems are very much like those experienced by survivors of COVID-19.
What is essential for the general public to understand is that recovery is a much longer process than they may expect. Individuals already impaired will “fall further” away from independence and may not return to their baseline. Perhaps we can change the adage and suggest that an ounce of prevention is worth far more than a pound of cure, and an additional pound or two of rehabilitation and almost recovery. The long-haulers are not limited to COVID-19; they have been with us all along. COVID-19 just shone a light on a problem physicians just weren't discussing.
[1] “feeding, toilet use, bowel and bladder control, grooming, dressing, bathing, mobility, stair climbing, and transfer from bed to chair and back.”
Source: Persistent Functional Decline Following Hospitalization with Influenza or Acute Respiratory Illness Journal of the American Geriatrics Society DOI: 10.1111/jgs.16950

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


