
Prisons and nursing homes share some transmission characteristics for COVID-19. Both have isolated, vulnerable populations, although nursing home populations are far more vulnerable. Both have experience with infectious disease outbreaks among their populations, more typically tuberculosis among prisoners. And both have a “vector of disease” living primarily in the community-at-large, but “piercing the membrane of the prison daily as they go to and from work” – we call those individuals guards in the one setting and nursing staff in the other.
The current study used data from the federal Bureau of Prisons (BOP) from March to December 2020, at which time the tools for intervention were non-pharmacologic – social distancing and masks. The BOP is the centralized administration for 137 federal prisons, including detention centers, medical centers, and minimal- to high-risk facilities. The researchers eliminated facilities that had insufficient information on staff-to-inmate staffing, transfer centers with “non-incarceration operational functions,” or those managed by private companies. Sixty-four prisons remained – all functioning as “traditional” prisons across 27 states. The researchers also had information on the demographics and the incidence of COVID-19 in the community.
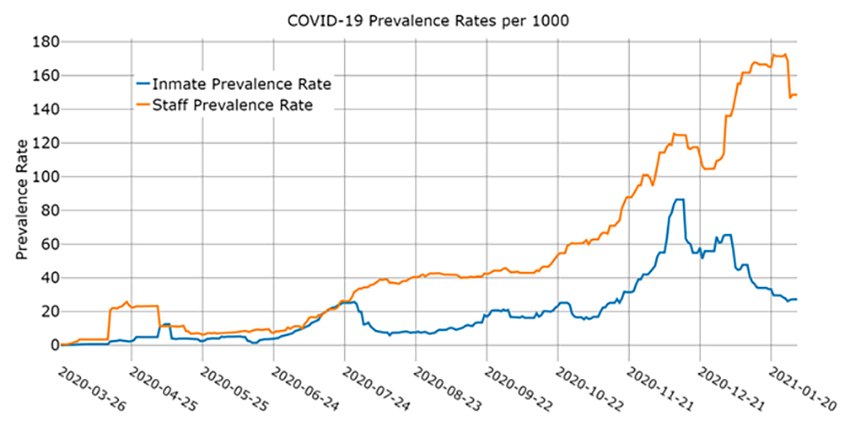
This graphic captures the key findings. Infections among prisoners lagged behind infections among guards, consistent with the roughly five days that COVID is infectious before becoming symptomatic. The incidence of infections among guards was higher than among the prisoners. The quantitative analysis found that for every 1% increase in community prevalence, there was a 0.65% increase among prisoners; a 1% rise among guards resulted in a 0.24% increase among inmates. Prisoners, while isolated from the community, are protected from the community’s infectious diseases.
The data on mask use remains uncertain. There were reduced infections with masks, but a positive association persisted in COVID-19 cases in the community and guards and transmission to the prisoners.
“The effectiveness of a policy is only as good as how the policy is written and then implemented. Discretionary components of policy …. allow for variations in implementation, potentially undermining the effectiveness of the policy.”
- There are “reciprocal dynamics” between prison guards, the at-large community, and the prison populations.
- The correctional officers are exposed to the at-large community's infectivity, subsequently transmitting this within the prison population - even when that transmission is not apparent - from the asymptomatic to the asymptomatic.
- The mask mandate by the BOP brought about only a small decline in cases. While many prisons had specific infection control policies on the books, “US prisons did not enact staff-specific policy for months.”
As the Delta variant plays havoc with our plans to reopen society, we need to consider this study. Most directly, it enforces what we have learned about the spread of COVID-19 in nursing homes – many of the cases resulted from community transmission through nursing home staff to the nursing home residents. When the staff is infectious, the frail and elderly - the kindling of the nursing home, become the wildfire. In many instances, the transmission was from the asymptomatic; that is why wearing a mask, even if vaccinated, has some value. The stealthy nature of COVID-19 rests upon asymptomatic spread.
The analogy between prisons and schools is not exact, except in the view of some students. Schools are more open; the students go home at the end of the day, so the prevalence of COVID-19 in the community is a reasonable measure of risk. More importantly, children are far more likely to be asymptomatic transmitters than the adults surrounding them. Schools, like prisons and nursing homes, can act as super-spreader locations. It very well may be that masks in school are more protective of the children’s teachers and parents than of the children themselves.
There is increasing evidence, from breakthrough infections, that our vaccines are very, but not entirely, protective. Vaccines are so protective that symptoms can be so mild or non-existent that asymptomatic spread continues. Masks are part of a “belt and suspenders” effort to mitigate COVID-19 in all its forms.
Source: Is There A Temporal Relationship Between COVID-19 Infections Among Prison Staff, Incarcerated Persons and the Larger Community in the United States? International Journal of Environmental Research and Public Health DOI: 10.3390/ijerph181.36873

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


