
I wrote about AstraZeneca’s vaccine problems a little over three weeks ago, mainly about the “unforced errors” in reporting. At that time, concerns about abnormal blood clots were being investigated and thought to be unanticipated but not abnormal, at least statistically. The situation seems to have changed.
The Background
Let’s talk for a minute about platelets, a cellular element that circulates in our bloodstream and provides the scaffolding for the formation of clots. If you view our arteries and veins as a plumbing system, you know that leaks, small or large, are bound to happen. In those instances, and they occur throughout our day, platelets plug the leak as other clotting factors arrive to form a clot and then “patch” the hole.
One of the manifestations of COVID-19 has been developing clots, frequently small and causing discoloration of your toes. Because the virus seems to inflame the lining of our arteries, platelets are activated in response. Some of these platelet clumps dissolve; others get lodged in our capillaries, creating that discoloration. In any event, this enhanced clotting can lead paradoxically to our platelet count dropping to the point where we can no longer form clots at all and begin to bleed. The medical term for this is disseminated intravascular coagulation or DIC, and it is a frequent manifestation of severe bacterial infections.
“HIT is thought to be the result of an immune reaction to complexes formed when negatively charged heparin molecules bind to a positively charged protein called platelet factor 4, which is important for clotting. The result is activation of platelets, kicking off a chain reaction.” Nature
DIC can also paradoxically be seen, rarely, in patients given heparin, a blood-thinner. It seems that in some individuals, heparin induces an autoimmune response, call Heparin-Induced Thrombocytopenia or HIT, which sets off the same increased clotting and depletion of platelets. Scientists are pursuing this reaction as the underlying basis for the clotting noted with the AstraZeneca vaccine.
Shifting Data and Denominators
The European Medicines Agency (EMA), the EU’s answer to the CDC, has been carefully following the start and stop roll-out of the vaccine in the EU. On March 8th, there had been reports of 37 blood clots in 17 million vaccine dosages – a vanishingly small percentage. Based on the incidence of reported blood clots in the general population, roughly 2/1000 individuals, the vaccine’s 37/17,000,000 seems to be random. The EMA noted the finding and stated that the benefits of vaccination far outweighed this seemingly “random” event.
But more cases have come forward. Late in March, Germany identified 31 cases, 29 of which were in women, and the UK reported 79 cases, 51 in women, 28 in men. Of the nineteen associated deaths in the UK, two-thirds were among women. Looking at those numbers, your immediate response would be that women were more susceptible. If you were a physician, you might jump there even more quickly, knowing that women are more inclined to clotting already because of their endogenous estrogen or exogenous estrogen from birth control pills.
This is a moment when you need to know the denominator. As it turns out, more women than men have been vaccinated, and when that is accounted for, women are no more likely to develop this disorder than men. As the scientists continued to rummage through the sparse data, they also noted that most of these cases involve those under age 60. That might make sense if an autoimmune response is the culprit; younger people have more robust immune responses than the elderly.
Messaging in the EU
The EMA did not change its guidance – the rare cases of clotting did not outweigh the benefit. But the UK’s Joint Committee on Vaccination and Immunisation felt differently and indicated that those under age 30 should opt for a different vaccine. Same data, different conclusions – neither wrong nor right.
The EU is not the US. The EU consists of 28 countries, 24 languages, and to be truthful, many of those countries have been fighting with one another for centuries. If you think the US messaging on COVID-19 is mixed, imagine trying to develop a single EU message. As a result, each country has stopped and re-started using the AstraZeneca vaccine in its own way and time. That can cause a great deal of mistrust. Transparency about the decision-making process is helpful, but it won’t change minds when the UK says one thing and a host of EU countries same something else.
Assessing Risk
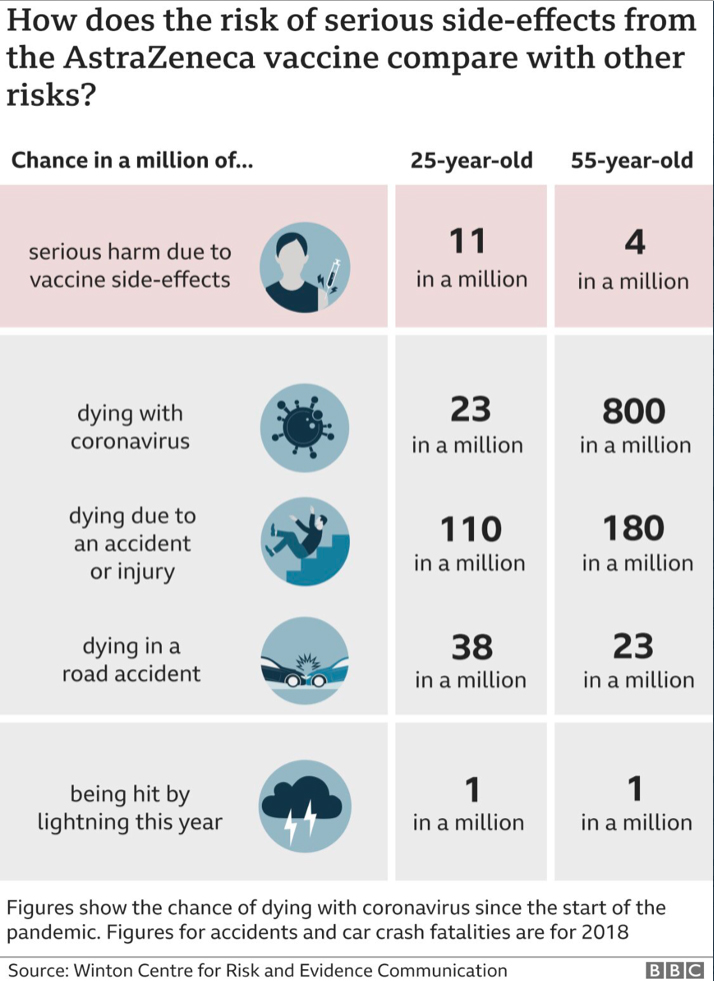
Evaluating risk is tricky, more so when the heightened concern leads you to jump on day-to-day data and not allow for cases to accumulate. There is the problem of correlation confused with causation. The early data suggested that clotting correlated with gender, the data just a few weeks later, indicated that it was not causative. And there is our inability to understand tiny and huge numbers. 37 cases in 17 million vaccinations that is 0.0002% - what does that number mean? This infographic may help.
Finally, when we think about risk, especially to ourselves, it is more an emotional response than an analytic one. It is tough to accept the AstraZeneca “jab” if you feel you are at risk, no matter how eminent an authority tells you otherwise.

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


